
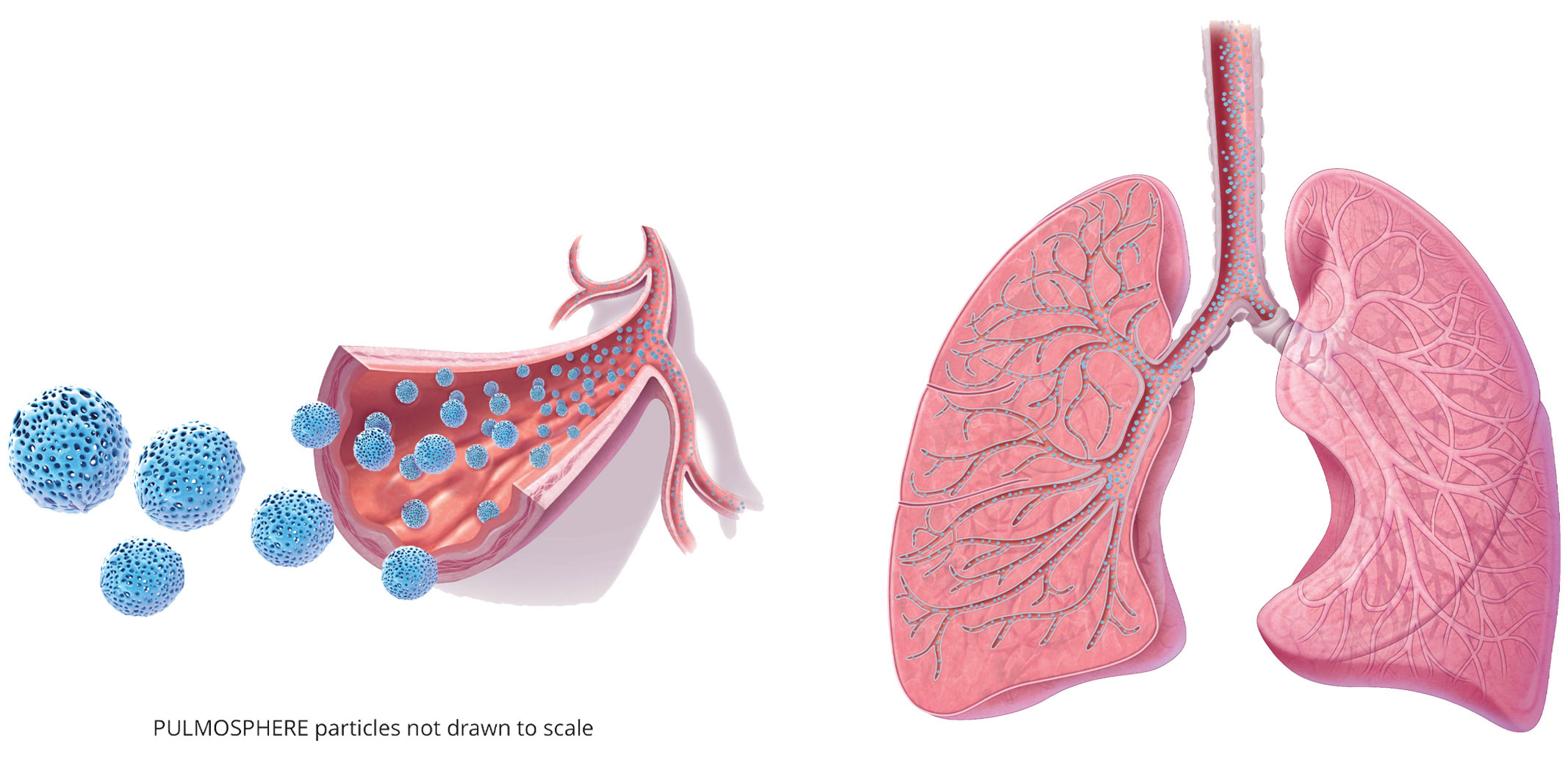
Tobramycin inhalation powder is delivered to both the central and peripheral airways.1
PULMOSPHERE® Technology
TOBI PODHALER delivers unique PULMOSPHERE powder particles which are1
- Low in density
- Light and porous
- Particle size: median geometric diameter is 1.7-2.7 μm
- Low energy is required to disperse the particles†
PULMOSPHERE are spherical particles, with pores that reduce the contact surface area between them and thus diminish the tendency to agglomerate. Particles are smaller than 5 μm, thus preventing deposition in the oropharynx and enabling the drug to be delivered successfully to the airway and alveoli. This technology enables rapid drug release using a device that requires little additional energy.
†The lung deposition fraction of PULMOSPHERE particles was evaluated utilizing gamma scintigraphy images in healthy volunteers.1Watch a video on PULMOSPHERE Technology
Watch a video on PULMOSPHERE Technology.
A closer look at PULMOSPHERE® Technology for TOBI® PODHALER®: Tobramycin Inhalation Powder. Please watch the Important Safety Information following this video. Please see accompanying Full Prescribing Information available on the site.
Indication: TOBI PODHALER (Tobramycin Inhalation Powder), 28 milligrams per capsule is indicated for the management of cystic fibrosis patients with Pseudomonas aeruginosa. Safety and efficacy have not been demonstrated in patients under the age of 6 years, patients with forced expiratory volume in 1 second (FEV1) <25% or >80% predicted or patients colonized with Burkholderia cepacia.
Select Important Safety Information - TOBI PODHALER is contraindicated in patients with known hypersensitivity to any aminoglycoside.
TOBI PODHALER is the first and only FDA approved inhaled antibiotic for Pseudomonas aeruginosa that utilizes a dry powder form.
The development of the TOBI PODHALER begins with its PULMOSPHERE technology. The active ingredient in TOBI PODHALER, tobramycin sulfate is mixed with non-active components in an emulsion which is subjected to spray drying. During initial drying, water evaporates leaving a concentrated droplet, wherein, tobramycin readily diffuses to the center of the droplet. With further drying, excipients form a shell on the surface of the droplet. Then lipid evaporates, leaving pores behind in the particle.
Pulmospheres are spherical particles with a median geometric diameter of 1.7 to 2.7 micrometers, with pores that reduce the contact surface area between them and thus diminish the tendency to agglomerate or clump. The smaller size of PULMOSPHERE particles enables the drug to be delivered with a high level of efficiency to the central as well as peripheral airways. Each PULMOSPHERE is engineered to carry approximately 60% of active drug, making it feasible to administer the required tobramycin dose via twice daily inhalation.
In a clinical trial, each dose of TOBI PODHALER was able to be administered in an average of 2-7 minutes. Due to TOBI PODHALER’s dry powder form, there is no nebulizer power source or refrigeration needed. TOBI PODHALER is portable with a compact, lightweight design, and cleanup is as simple as wiping the mouthpiece with a clean dry cloth. No washing, drying, or disinfection required.
The PODHALER device was designed specifically for the delivery of engineered PULMOSPHERE particles. There are three primary pieces to the PODHALER device. The mouthpiece, the chamber where the capsule goes, and the blue button, which activates a sharp pin to pierce the capsule and access the PULMOSPHERE particles.
In summary, TOBI PODHALER’s low interparticle cohesive forces and smaller particle size allow for the necessary dispersibility during inhalation. So, the PULMOSPHERE Technology and the low resistance inhaler, together, create the TOBI PODHALER - the first FDA approved dry powder inhaled antibiotic for Pseudomonas aeruginosa.
Please continue to watch for the Important Safety Information about TOBI PODHALER (Tobramycin Inhalation Powder).
Indication: TOBI PODHALER (Tobramycin Inhalation Powder) 28 milligrams per capsule is indicated for the management of cystic fibrosis patients with Pseudomonas aeruginosa. Safety and efficacy have not been demonstrated in patients under the age of 6 years, patients with forced expiratory volume in 1 second (FEV1) <25% or >80% predicted, or patients colonized with Burkholderia cepacia.
TOBI PODHALER is contraindicated in patients with known hypersensitivity to any aminoglycoside. Bronchospasm can occur with inhalation of TOBI PODHALER. Bronchospasm should be treated as medically appropriate. Caution should be exercised when prescribing TOBI PODHALER to patients with known or suspected auditory, vestibular, renal, or neuromuscular dysfunction. Ototoxicity, as measured by complaints of hearing loss or tinnitus, was reported by patients in the TOBI PODHALER clinical studies. Tinnitus may be a sentinel symptom of ototoxicity, and therefore the onset of the symptom warrants caution. Ototoxicity, manifested as both auditory and vestibular toxicity, has been reported with parenteral aminoglycosides. Vestibular toxicity may be manifested by vertigo, ataxia, or dizziness.
Cases of ototoxicity with aminoglycosides have been observed in patients with certain variants in the mitochondrially encoded 12S rRNA gene (MT-RNR1), particularly the m.1555A>G variant. Ototoxicity occurred in some patients even when their aminoglycoside serum levels were within the recommended range. Mitochondrial DNA variants are present in less than 1% of the general US population, and the proportion of the variant carriers who may develop ototoxicity as well as the severity of ototoxicity is unknown. In case of known maternal history of ototoxicity due to aminoglycoside use or a known mitochondrial DNA variant in the patient, consider alternative treatments other than aminoglycosides unless the increased risk of permanent hearing loss is outweighed by the severity of infection and lack of safe and effective alternative therapies.
Caution should be exercised when prescribing TOBI PODHALER to patients with known or suspected renal dysfunction. Nephrotoxicity was not observed during TOBI PODHALER clinical studies but has been associated with aminoglycosides as a class.
TOBI PODHALER should be used cautiously in patients with neuromuscular disorders, such as myasthenia gravis or Parkinson's disease, since aminoglycosides may aggravate muscle weakness because of a potential curare-like effect on neuromuscular function.
Aminoglycosides can cause fetal harm when administered to a pregnant woman. Patients who use TOBI PODHALER during pregnancy, or who become pregnant while taking TOBI PODHALER, should be apprised of the potential hazard to the fetus. The amount of tobramycin excreted in human breast milk is unknown. However, systemic absorption of tobramycin following inhaled administration is expected to be minimal. A decision should be made whether to discontinue nursing or TOBI PODHALER. TOBI may cause intestinal flora alteration. Advise a woman to monitor the breastfed infant for loose or bloody stools and candidiasis.
Patients receiving concomitant TOBI and parenteral aminoglycoside therapy should be monitored as clinically appropriate for toxicities associated with aminoglycosides as a class. Serum tobramycin levels should be monitored. Concurrent and/or sequential use of TOBI PODHALER with other drugs with neurotoxic, nephrotoxic, or ototoxic potential should be avoided. Some diuretics can enhance aminoglycoside toxicity by altering antibiotic concentrations in serum and tissue. TOBI PODHALER should not be administered concomitantly with ethacrynic acid, furosemide, urea, or mannitol.
In a clinical trial, the most commonly observed adverse events, with TOBI PODHALER occurring at a frequency of at least 10%, were cough, lung disorder, productive cough, dyspnea, pyrexia, oropharyngeal pain, dysphonia, hemoptysis, and headache.
Please see full Prescribing Information including patient information and instructions for use on www.tobipodhalerhcp.com.
Reference
- Geller DE, Weers J, Heuerding S. Development of an inhaled dry-powder formulation of tobramycin using PULMOSPHERE® Technology. J Aerosol Med Pulm Drug Deliv. 2011;24(4):175-182.
INDICATION
TOBI® PODHALER® (Tobramycin Inhalation Powder) 28 mg per capsule is indicated for the management of cystic fibrosis patients with Pseudomonas aeruginosa.
Safety and efficacy have not been demonstrated in patients under the age of 6 years, patients with forced expiratory volume in 1 second (FEV1) <25% or >80% predicted, or patients colonized with Burkholderia cepacia.
IMPORTANT SAFETY INFORMATION
TOBI PODHALER is contraindicated in patients with known hypersensitivity to any aminoglycoside.
Bronchospasm can occur with inhalation of TOBI PODHALER. Bronchospasm should be treated as medically appropriate.
Caution should be exercised when prescribing TOBI PODHALER to patients with known or suspected auditory, vestibular, renal, or neuromuscular dysfunction.
Ototoxicity, as measured by complaints of hearing loss or tinnitus, was reported by patients in the TOBI PODHALER clinical studies. Tinnitus may be a sentinel symptom of ototoxicity, and therefore the onset of this symptom warrants caution. Ototoxicity, manifested as both auditory and vestibular toxicity, has been reported with parenteral aminoglycosides. Vestibular toxicity may be manifested by vertigo, ataxia, or dizziness.
Cases of ototoxicity with aminoglycosides have been observed in patients with certain variants in the mitochondrially encoded 12S rRNA gene (MT-RNR1), particularly the m.1555A>G variant. Ototoxicity occurred in some patients even when their aminoglycoside serum levels were within the recommended range. Mitochondrial DNA variants are present in less than 1% of the general US population, and the proportion of the variant carriers who may develop ototoxicity as well as the severity of ototoxicity is unknown. In case of known maternal history of ototoxicity due to aminoglycoside use or a known mitochondrial DNA variant in the patient, consider alternative treatments other than aminoglycosides unless the increased risk of permanent hearing loss is outweighed by the severity of infection and lack of safe and effective alternative therapies.
Caution should be exercised when prescribing TOBI PODHALER to patients with known or suspected renal dysfunction. Nephrotoxicity was not observed during TOBI PODHALER clinical studies but has been associated with aminoglycosides as a class.
TOBI PODHALER should be used cautiously in patients with neuromuscular disorders, such as myasthenia gravis or Parkinson’s disease, since aminoglycosides may aggravate muscle weakness because of a potential curare-like effect on neuromuscular function.
Aminoglycosides can cause fetal harm when administered to a pregnant woman. Patients who use TOBI PODHALER during pregnancy, or who become pregnant while taking TOBI PODHALER, should be apprised of the potential hazard to the fetus. The amount of tobramycin excreted in human breast milk is unknown. However, systemic absorption of tobramycin following inhaled administration is expected to be minimal. A decision should be made whether to discontinue nursing or TOBI PODHALER. TOBI may cause intestinal flora alteration. Advise a woman to monitor the breastfed infant for loose or bloody stools and candidiasis.
Patients receiving concomitant TOBI and parenteral aminoglycoside therapy should be monitored as clinically appropriate for toxicities associated with aminoglycosides as a class. Serum tobramycin levels should be monitored.
Concurrent and/or sequential use of TOBI PODHALER with other drugs with neurotoxic, nephrotoxic, or ototoxic potential should be avoided. Some diuretics can enhance aminoglycoside toxicity by altering antibiotic concentrations in serum and tissue. TOBI PODHALER should not be administered concomitantly with ethacrynic acid, furosemide, urea, or mannitol.
In a clinical trial, the most commonly observed adverse events with TOBI PODHALER occurring at a frequency of at least 10%, were cough, lung disorder, productive cough, dyspnea, pyrexia, oropharyngeal pain, dysphonia, hemoptysis, and headache.
Please see Full Prescribing Information